
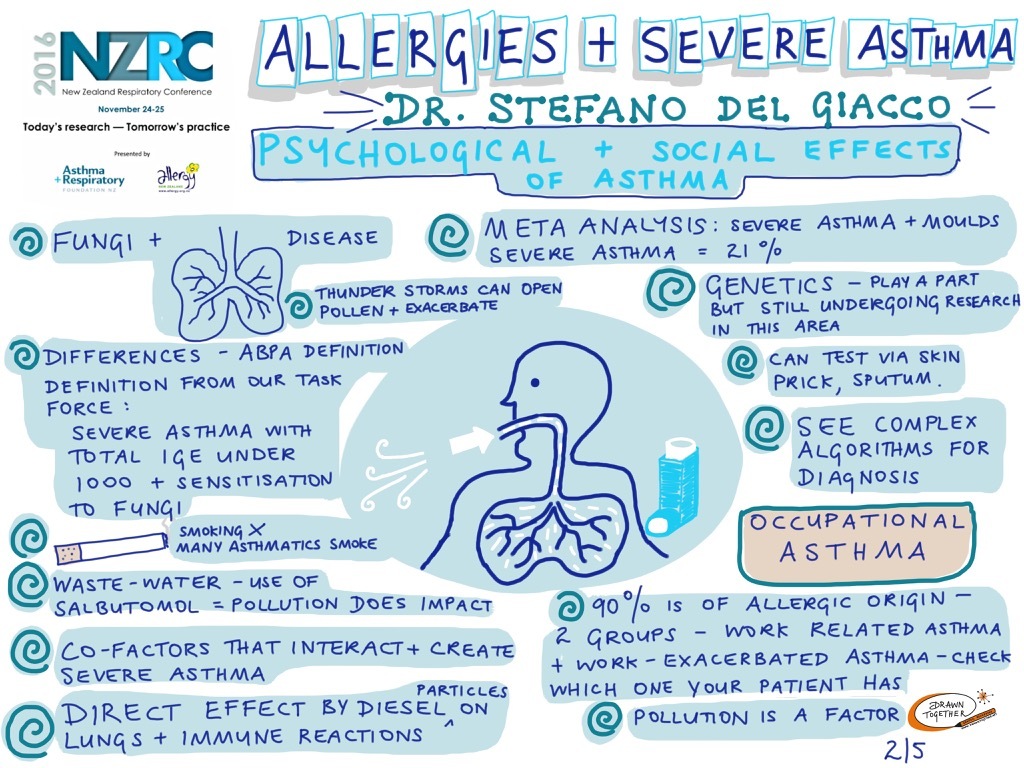
It is well recognised that atopic sensitisation is an important risk factor for asthma, both in adults and in children. However, the potential role of allergy in severe asthma is still under debate. The term “Severe Asthma” encompasses a highly heterogeneous group of patients who require treatment on steps 4–5 of GINA guidelines to prevent their asthma from becoming "uncontrolled", or whose disease remains "uncontrolled" despite this therapy. Epidemiological studies on emergency room visits and hospital admissions for asthma suggest the important role of allergy in asthma exacerbations, and allergic asthma in childhood is often associated with severe asthma in adulthood. A strong association of asthma exacerbations with respiratory viral infections has been demonstrated, and the interaction between viruses and allergy was shown to increase the risk of asthma exacerbations. Fungal allergy may also play an important role in severe asthma while cofactors such as smoking, pollution and work-related exposures must always be considered. In this plenary Stefano Del Giacco provided an overview about the role of allergy in severe asthma and the importance of the main co-factors in this link.
Watch the presentation here. (starts at 5.45min)
View the presentation visualisations here: Part 1, Part 2, Part 3, Part 4, Part 5
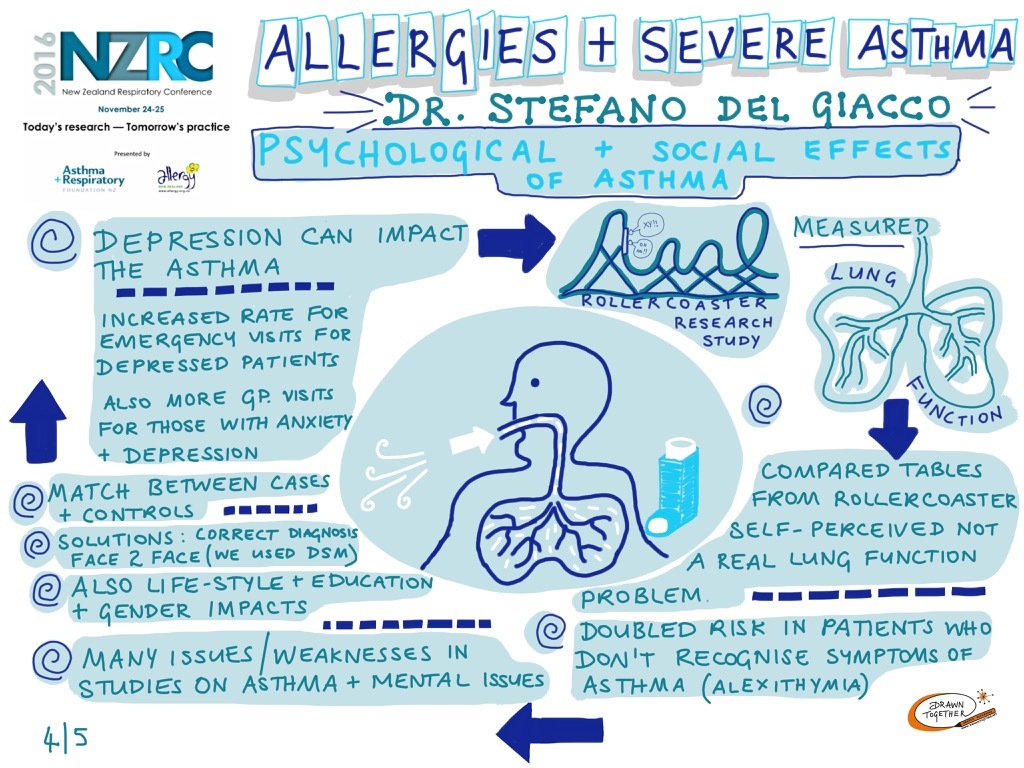
Asthma and psychological factors have been associated for centuries: Moses Maimonides (12th century), in his “Treatise on Asthma”, defined asthma as “difficulty of breathing or a pain in the chest” suggesting behavioural changes as one of the measures to cure it. The literature reports a significantly greater risk of depression, anxiety and/or mental disturbances in asthmatics, with important implications including symptom severity, reduced asthma control, lower quality of life, low therapy adherence, higher incidence of smoking, inactivity and obesity, increased use of healthcare services and therefore a rise in financial burden. However, the evidence gathered is not always univocal, and the association between asthma and affective disorders raised the debate on the true nature of this relationship, whether asthmatic disorders are associated with a higher risk of affective disorders, and/or vice versa, whether affective disorders increase the risk of developing asthma. Furthermore, fascinating hypotheses about the comorbidity between these disorders may suggest mutual pathogenetic mechanisms linked to the complex psycho-neuro-immunological pathways involving mainly pro-inflammatory cytokines and imbalance towards the Th2 T-cell response. In this plenary, Stefano Del Giacco will discuss about the links between asthma and psychiatric/psychological disorders and the importance of this comorbidity for the course of the illness, its prognosis and response to therapy.
Watch the presentation here. (starts at 37.15)
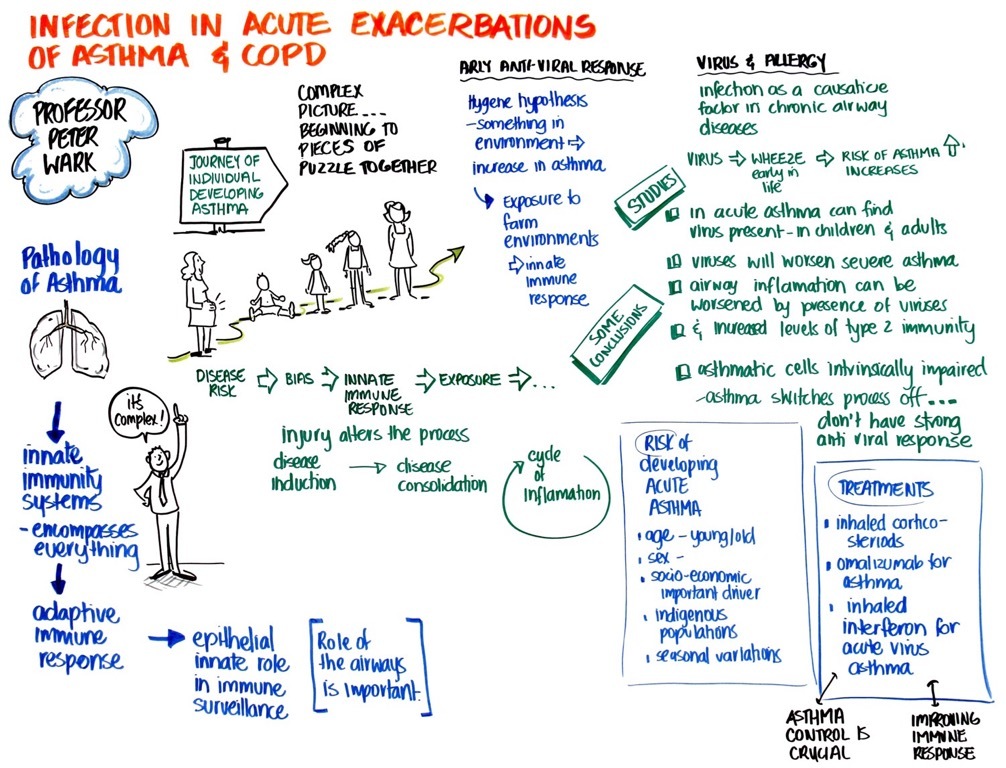
Review epidemiology infection, airways disease and the impact of infection. Review why people with asthma and COPD susceptible to infection. This session will also explore prevention and treatment including options for the future.
Watch the presentation here. (starts at 2.00 mins)
View the presentation slides here.
View the presentation visualisation here.
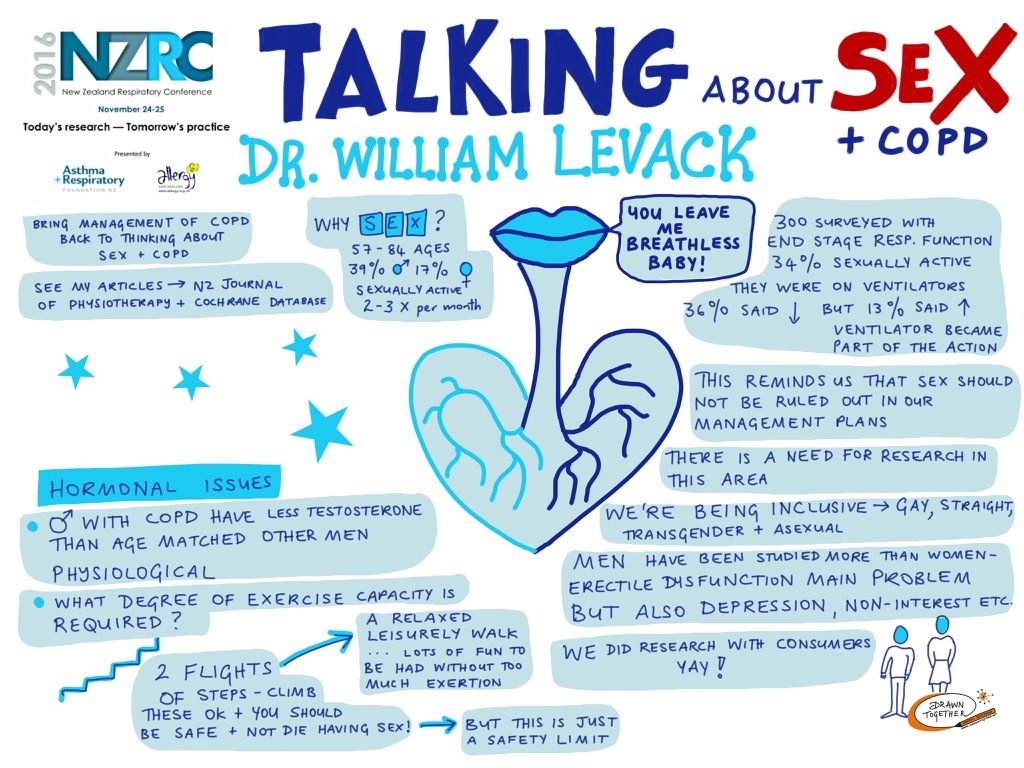
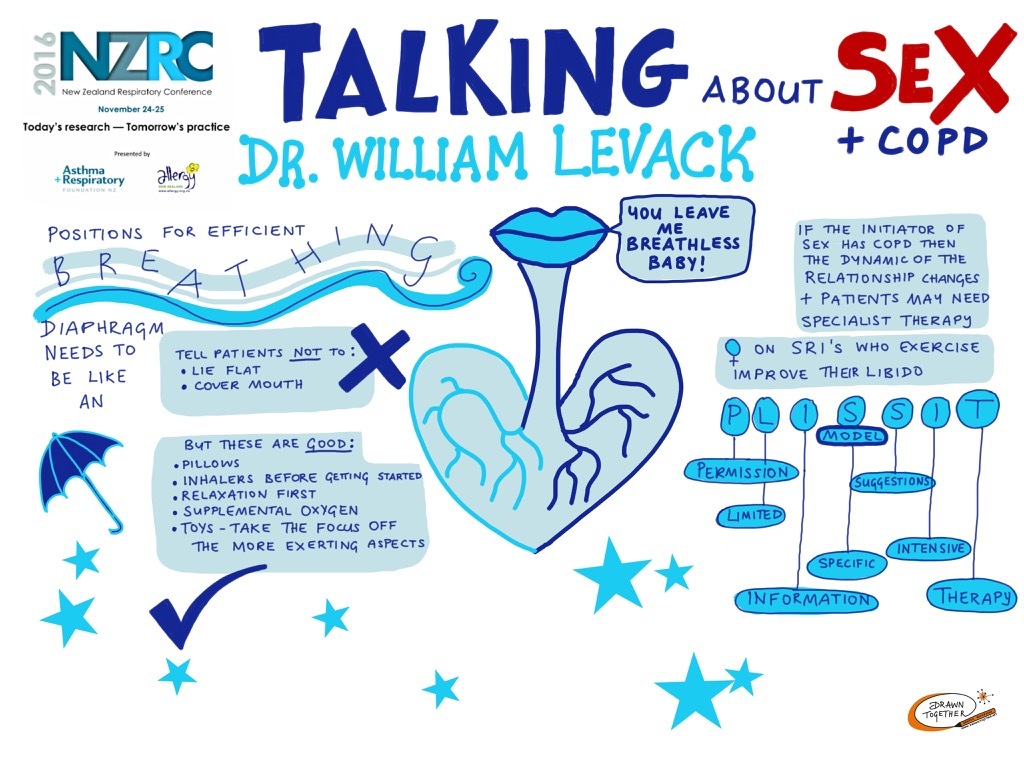
Chronic obstructive pulmonary disease (COPD) is the fifth leading cause of years with disability worldwide. Management of COPD is therefore not just about survival; it is also about helping people with COPD live well, maximising quality of life in spite of the chronic nature of their condition. In this regard, sexual wellbeing is potentially an important, but often neglected, aspect of disease management. The aim of this session is to provide an overview of current knowledge on sexual wellbeing for people with COPD and the possible role of health professionals in helping people with COPD maintain or regain active and enjoyable sex lives. This session draws on a structured review of the literature investigating issues of prevalence, causes, and management of sexual problems associated with COPD. In general, people with COPD seem to experience more sexual problems on average than the general population, with these issues arising from hormonal, physiological, psychological, sociological, and pharmaceutical factors. In additional to medical interventions to aid sexual function, health professionals can provide support for people with COPD and their sexual partners regarding their sex lives through the provision of exercise therapy; advice on positioning, breathing efficacy, and energy conservation during sexual activity; and via education on sexuality and chronic condition management. The PLISSIT model provides a robust framework for helping therapists clarify their scope of practice when engaging with people who have COPD on matters to do with sexuality. The research on sexuality and COPD is grossly underdeveloped considering the potential importance of the subject. Regardless of age or severity of symptoms, people with COPD are capable of leading full and satisfying sex lives should they wish to do so. Doctors, nurses, and allied health professionals all can have a role in providing information and solutions to support them in this endeavour.
View the presentation here.
View the presentation slides here.
View the presentation visualisations here and here.
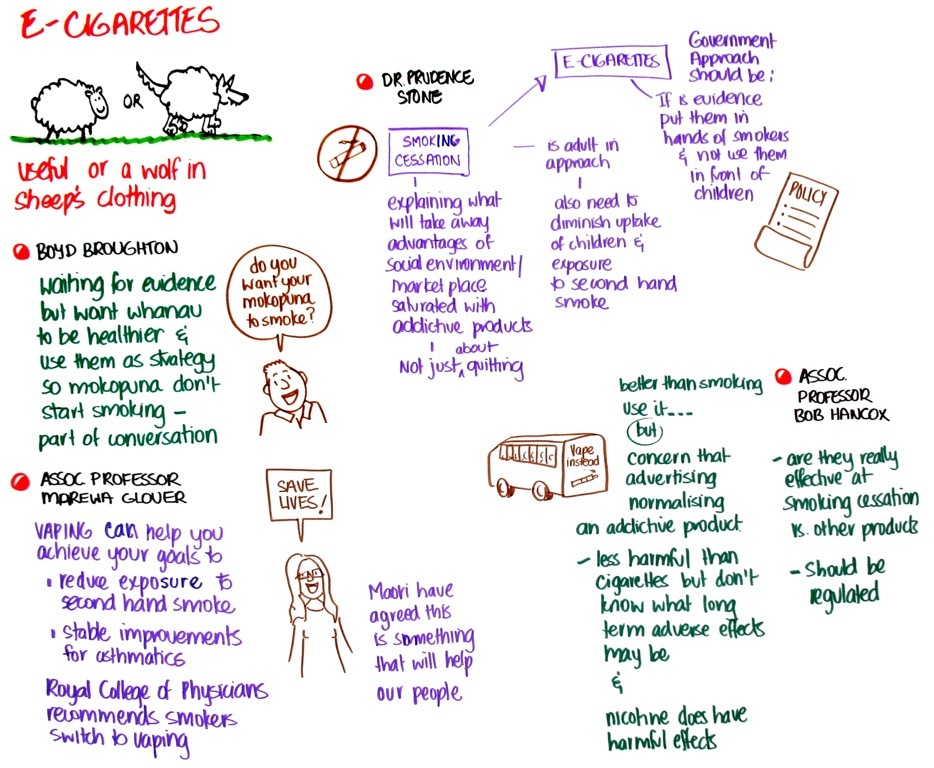
Panel chair: Professor Peter Wark
Panel: Dr Prudence Stone, Associate Professor Marewa Glover
View the discussion here. (starts at 1.16.10)
View the discussion visualisations here and here.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}